Mice homozygous for the lymphoproliferation mutation (Faslpr) exhibit autoimmune disease that closely resembles human systemic lupus erythematosus (SLE).
Induction
Spontaneous onset.
Disease Parameters/Progression
Systemic autoimmunity, lymphadenopathy associated with proliferation of aberrant T cells, immune complex glomerulonephritis and arthritis start at approximately 10-12 weeks of age. The disease significantly affects both female and male MRL/Mp-Faslpr mice; female mice die at an average age of 17 weeks of age and males at 22 weeks1, 7.
Dosing Paradigms
Developing (Prophylactic) – Begin dosing at around 9 weeks of age and continue until necropsy (around week 20).
Semi-Established (Semi-therapeutic) – Begin dosing at around 12 weeks of age and continue until necropsy (around week 20).
Established (Therapeutic) – Begin dosing at around 15 weeks of age and continue until necropsy (around week 20).
Route of administration: SC, PO, IP, IV
Clinical Assessment
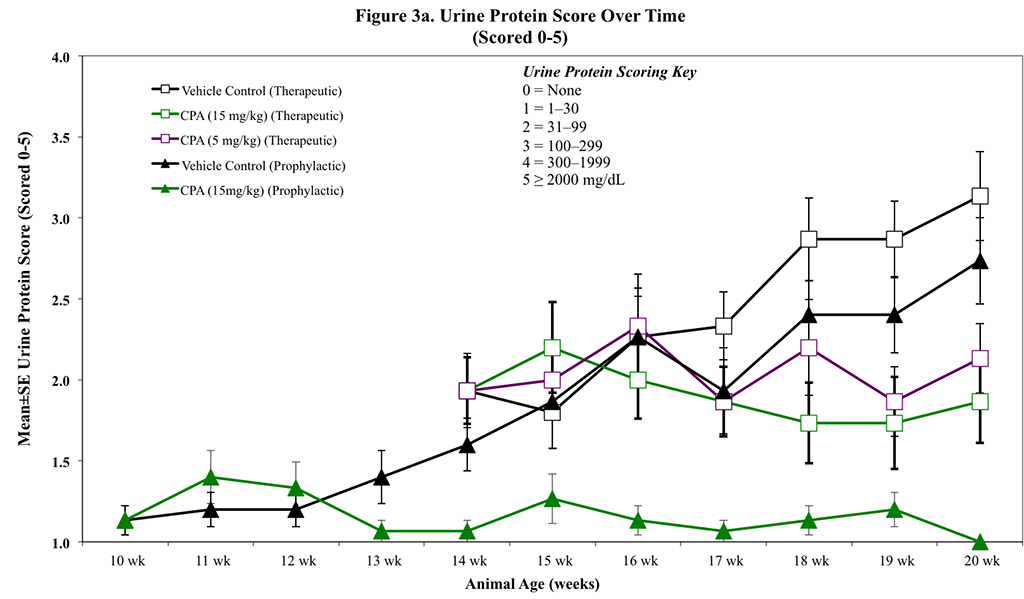
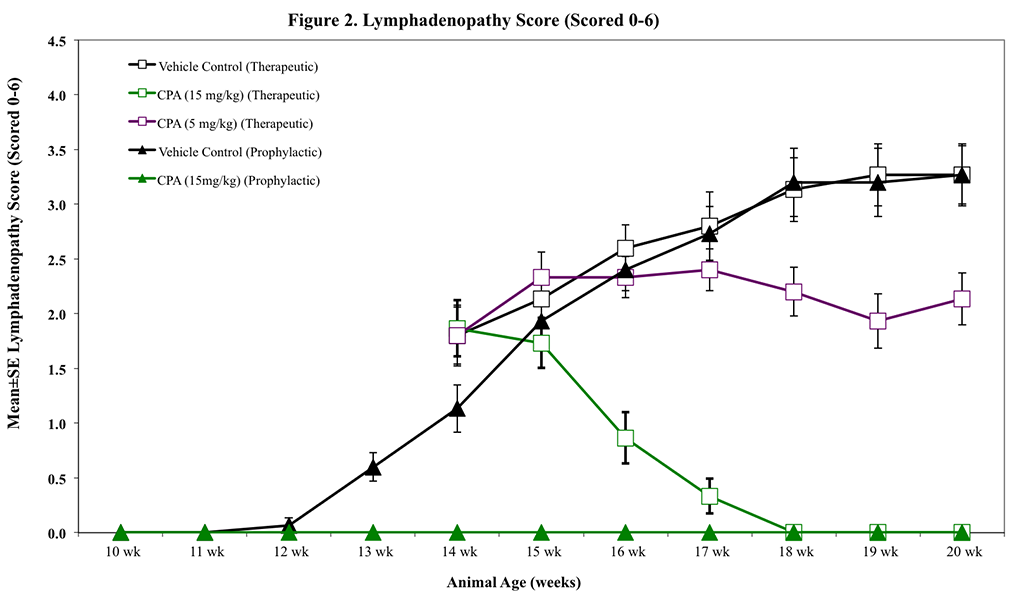
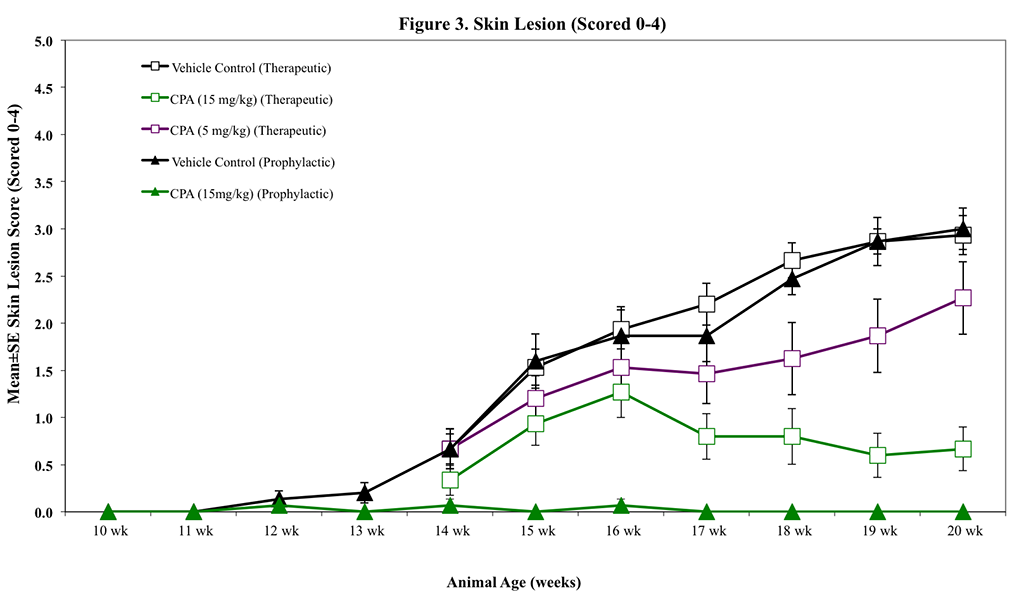
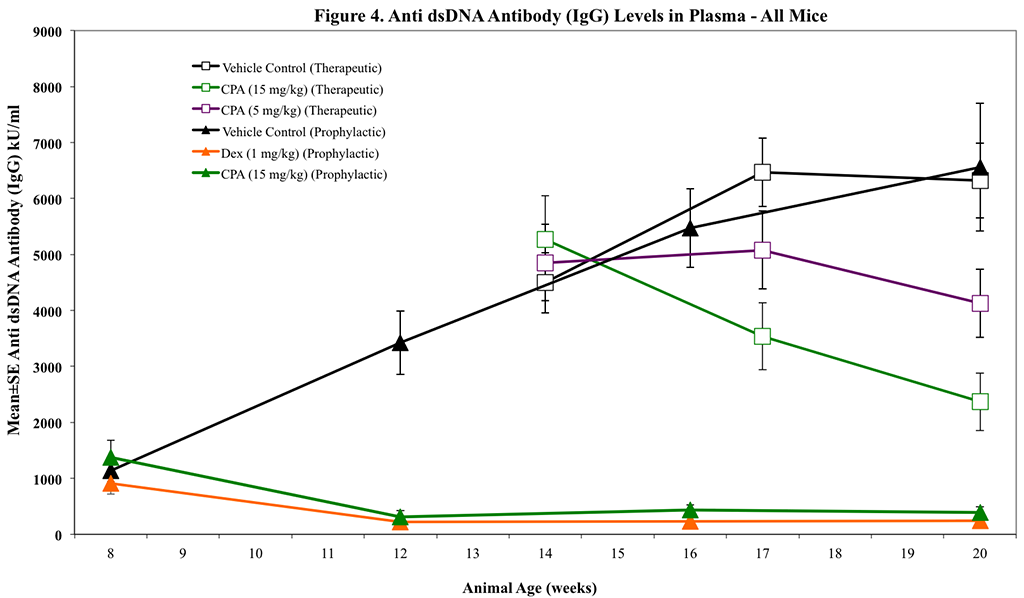
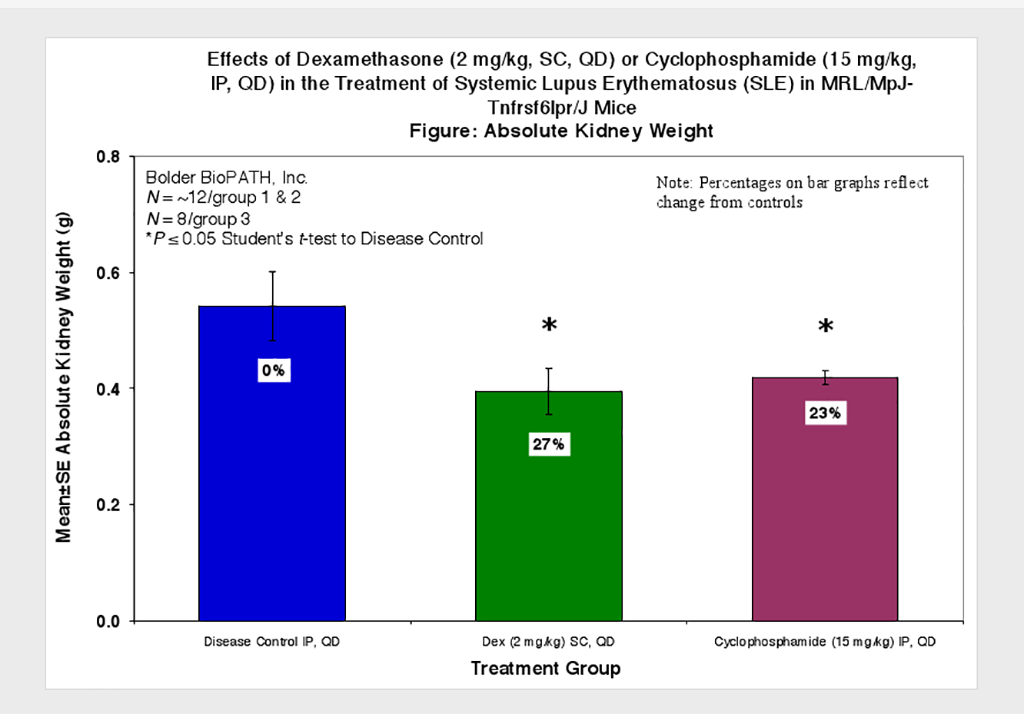
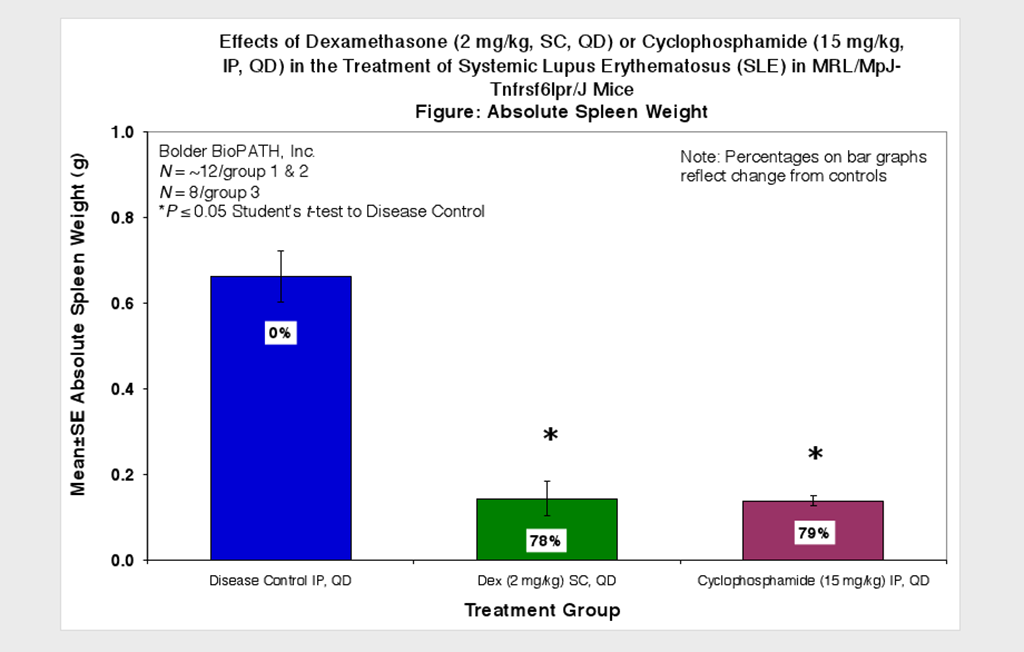
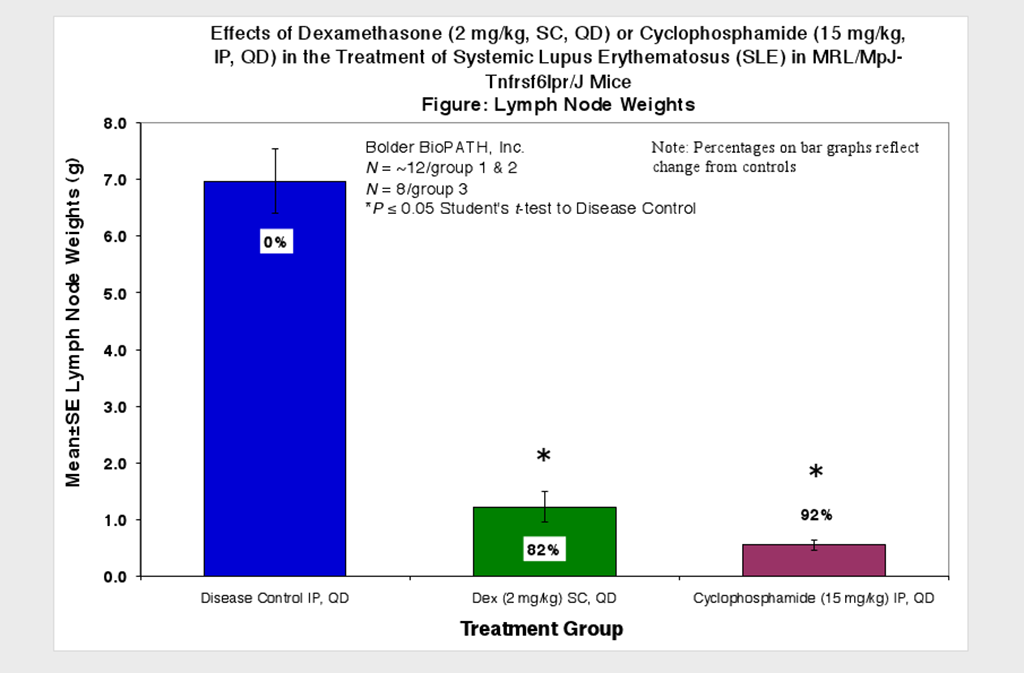
Animals are observed daily for significant clinical signs, moribundity and mortality. Body weights and proteinuria are recorded weekly and at scheduled termination points. Urine protein is measured using Albustix test strips (Siemens). Lymphadenopathy (bilateral cervical, brachial/axillary, and inguinal) and skin lesions (when present) are also scored weekly and at termination (see Scoring Keys below). Plasma samples for anti-dsDNA ELISA can be collected periodically at desired time points. At necropsy, kidneys (paired), spleens and lymph nodes are collected and weighed.
0 = None. 1 = Small (<1 cm diameter combined) at one bilateral site. 2 = Small at two bilateral sites. 3 = Small at three bilateral sites. 4 = Large (>1 cm combined) at one bilateral site and small at two. 5 = Large at two bilateral sites and small at one. 6 = Large at all three bilateral sites.
Skin Lesion Scoring Key:
0 = None. 1 = 1 or 2 small (2-4 mm in length). 2 = Lesion(s) larger than a “1”, but with total area <0.5 cm2. 3 = Lesion(s) with total area >0.5, but <1.0 cm2. 4 = Lesion(s) with total area >1.0 cm2.
Histopathological Assessment
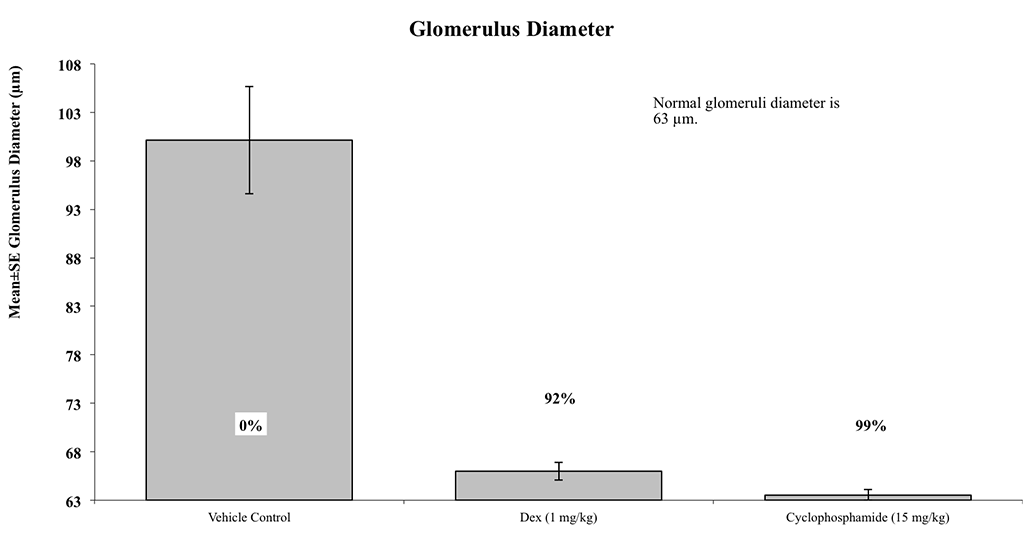
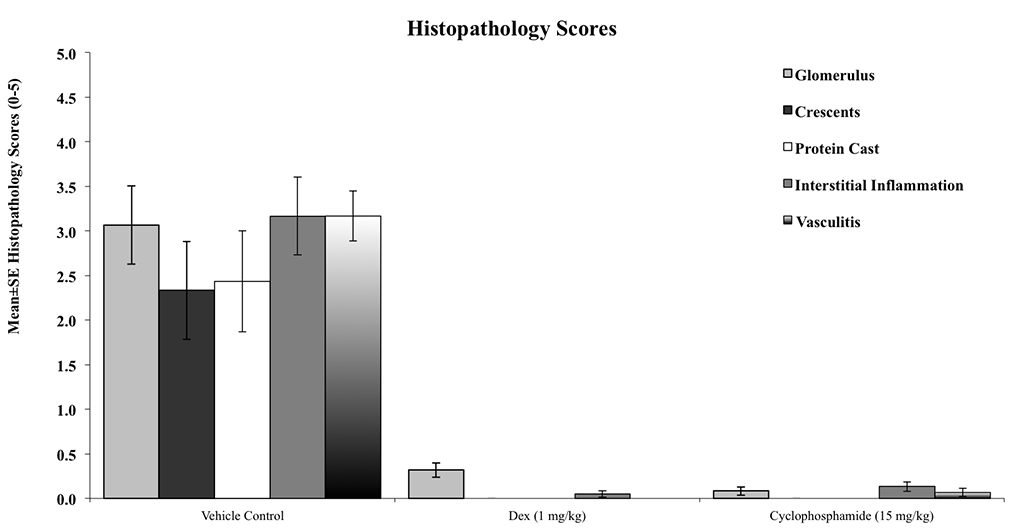
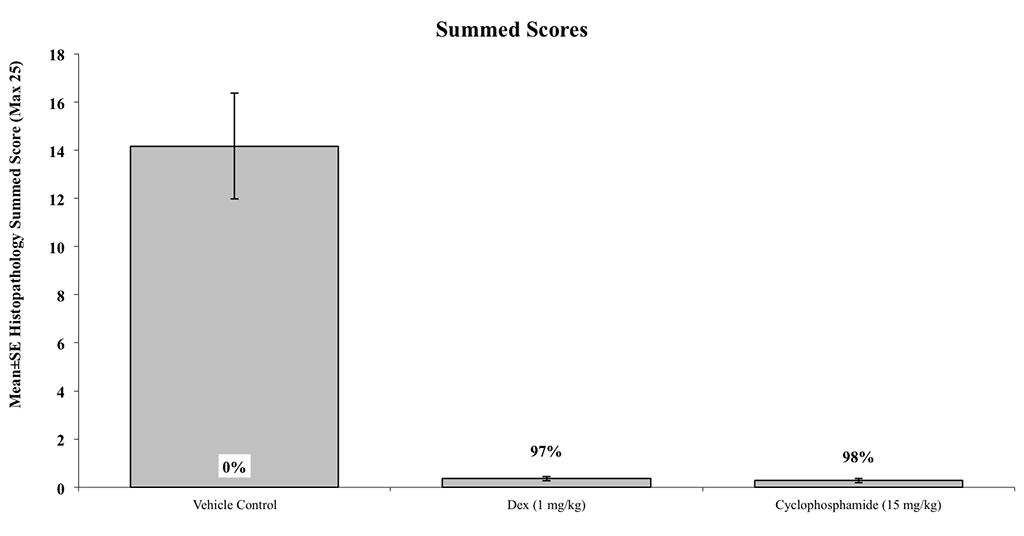
Kidneys from all surviving animals are examined microscopically by a board certified veterinary pathologist (Dr. Alison Bendele) and scored for: glomerular diameters and crescents, tubular protein casts, interstitial inflammation, and vasculitis, according to these methods.
Sample Data (Click on image to enlarge):
Notes:
In addition to multiple underlying genetic factors contributing to the pathogenesis of SLE in MRL/lpr mice, a single genetic mutation that leads to aberrant Fas transcription accelerates the disease’s progression. As in human lupus, SLE in MRL/lpr mice is biased in favor of females, although it significantly affects males as well1. Clinical manifestations of SLE in this model include hyperactive B and T cells, high titers of several autoantibodies including antineutrophil antibodies (ANA) and anti-dsDNA antibodies2, defective clearance of immune complexes, and fatal renal disease (glomerulonephritis, interstitial nephritis, vasculitis, and proteinuria). MRL/lpr mice differ from other strains in that they have the highest titers and largest array of auto-antibody specificities, and they develop antibodies against the nuclear components Smith (Sm) and ribonucleoprotein (RNP). A proportion of MRL/lpr mice also develop skin rash, inflammatory arthritis, and immunoglobulin (Ig) M rheumatoid factors. Lymphoid hyperplasia, which is not a feature of human SLE, is exhibited by MRL/lpr mice and this can confound histopathology3. The speed of the disease in the MRL/lpr strain is sufficiently rapid to be efficient in testing new therapies and sufficiently slow to dissect the pathogenesis of the disease4–6.
Optional Endpoint
PK/PD blood collections
Cytokine/chemokine analysis via Luminex(R)
Anti-dsDNA Ab and other sandwich ELISAs
CBC/clinical chemistry analysis
Soft tissue collection
Histopathologic analysis
Immunohistochemistry analysis
FACS analysis of spleen cell populations
References
Perry D, Sang A, Yin Y, et al. Murine models of systemic lupus erythematosus. J Biomed Biotechnol, 2011. doi:10.1155/2011/271694.
Rottman JB, and Willis CR. Mouse models of systemic lupus erythematosus reveal a complex pathogenesis. Vet Pathol, 2010;41:664. doi:10.1177/0300985810370005.
Theofilopoulos AN, Dixon FJ. Etiopathogenesis of murine SLE. Immunol Rev, 55: 179, 1981.
Wada T, Schwarting A, Chesnutt MS, Wofsy D, Rubin Kelley V. Nephritogenic cytokines and disease in MRLFas(lpr) kidneys are dependent on multiple T-cell subsets. Kidney Int, 59:565–578, 2001.