Rat adjuvant arthritis (AIA) is an experimental model of polyarthritis that has been widely used for preclinical testing of numerous anti-arthritic agents, which are either under preclinical or clinical investigation, or are currently used as therapeutics in this disease2-4. The lesions in adjuvant arthritis are somewhat less analogous to those seen in human RA than are the lesions of type II collagen arthritis in that there is less extensive pannus associated cartilage destruction. However, adjuvant arthritis has been used much more extensively for pharmaceutical testing and therefore more data exists for comparison in humans.
Induction:
Rats are injected with 100 µL of FCA/LA (60 mg/mL) at the base of the tail on day 0.
Disease Parameters:
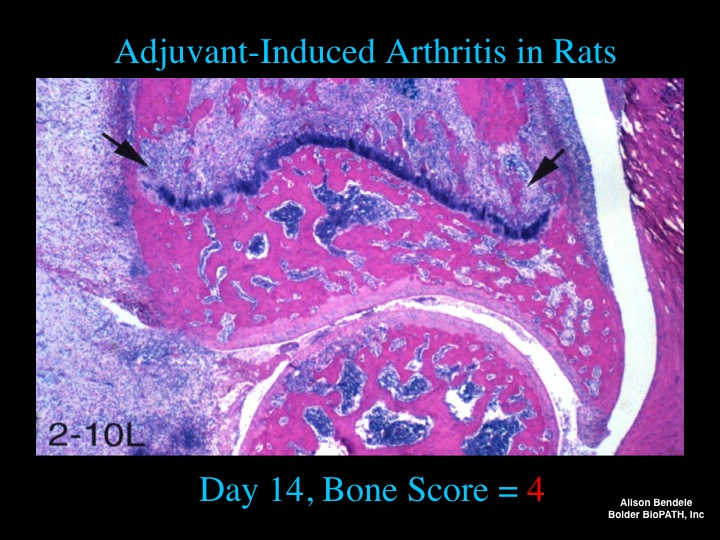
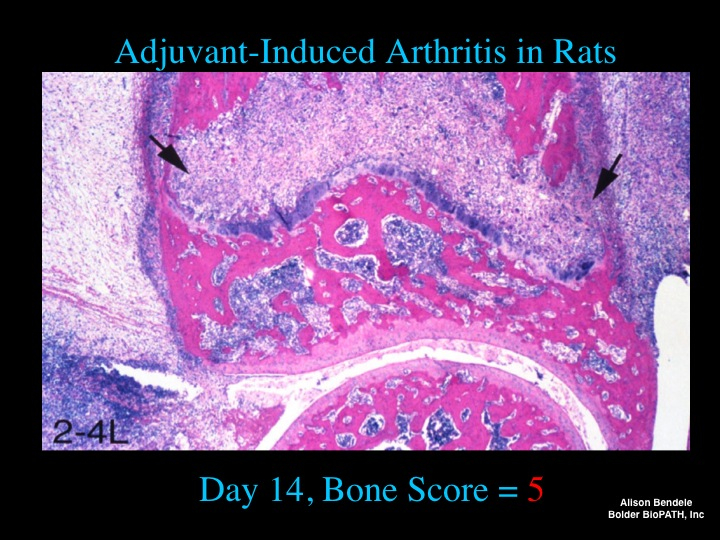
The hallmarks of this model are reliable onset and progression of robust, easily measurable, polyarticular inflammation, marked bone resorption and periosteal bone proliferation. Cartilage destruction occurs but is disproportionally mild in comparison to the inflammation and bone destruction that occurs. Clinical evidence of arthritis occurs on day 9 or 10 after injection of adjuvant.
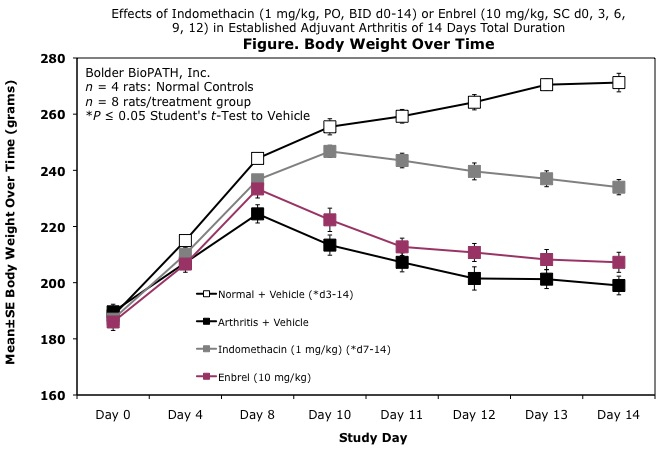
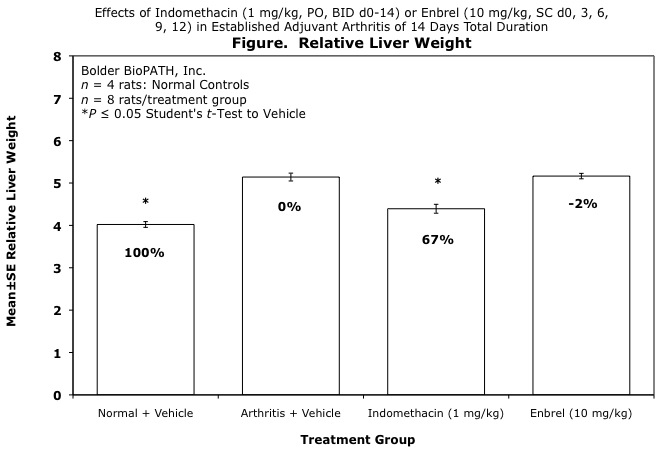
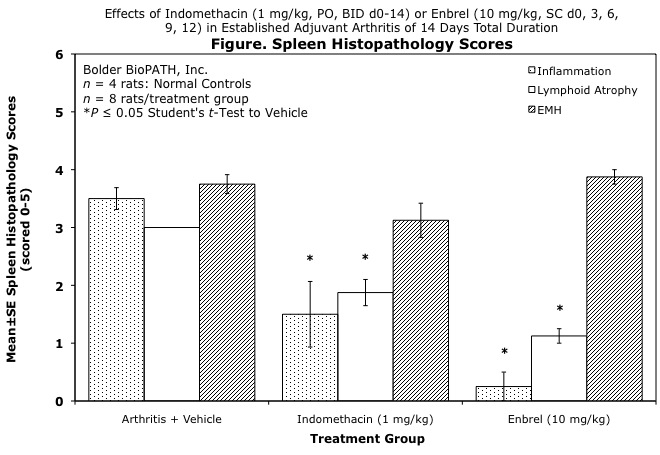
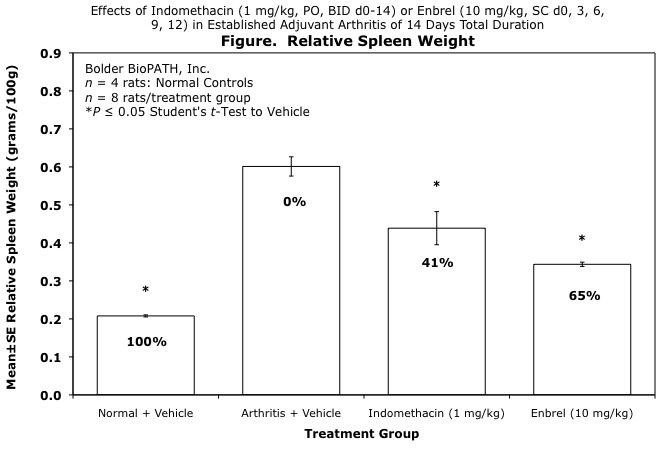
Additionally, splenomegaly occurs as a result of profound induction of extramedullary hematopoiesis in the red pulp in conjunction with pyogranulomatous inflammation in the red pulp and capsule. These changes are usually in association with mild to marked lymphoid atrophy. Ideally, an agent active in adjuvant disease should restore the spleen weights and morphology to normal as is the case with methotrexate treatment. Hepatomegaly also occurs as a result of hypertrophy of hepatocytes and should be beneficially affected by treatment. Also fairly consistently present in these animals is an anterior uveitis which may be histologically evaluated for treatment effects.
Dosing Paradigms:
- Developing (Prophylactic) – Begin dosing on study day 0 and continue until necropsy on day 14.
- Semi-Established (Prophylactic) – Begin dosing on study day 6 and continue until necropsy on day 14.
- Established (Therapeutic) – Begin dosing on study day 8 and continue for 7 to 11 days.
Clinical Assessment:
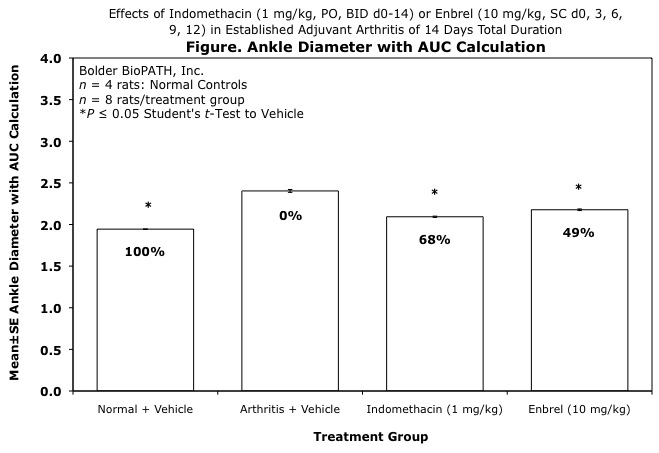
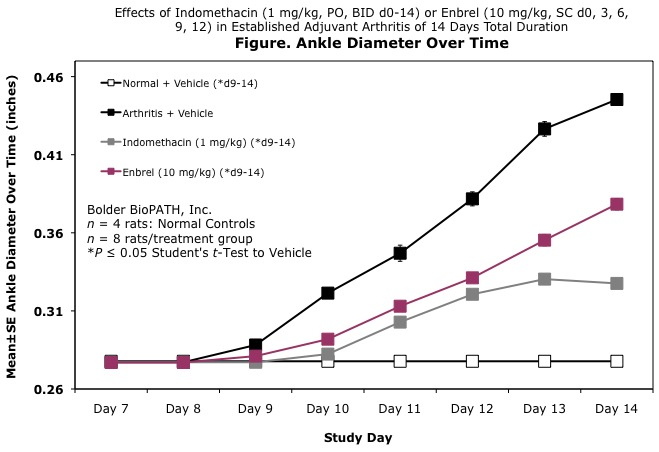
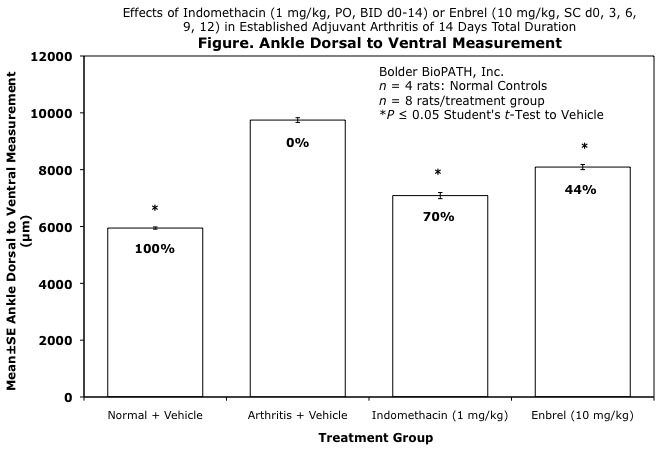
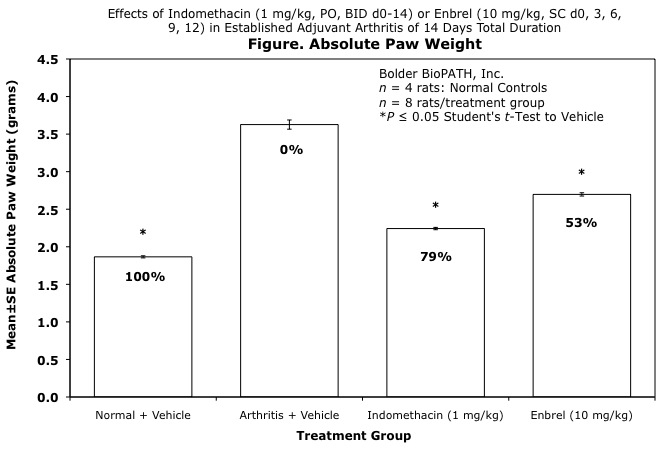
To assess disease progression, caliper measurements of ankle joint width or volume using a water displacement device are done prior to the onset of arthritis, and then every other day until the study is terminated. At termination, the tibiotarsal joint is transected at the level of the medial and lateral malleolus for determination of paw weights as another measure of inflammation or its inhibition.
Histopathological Assessment:
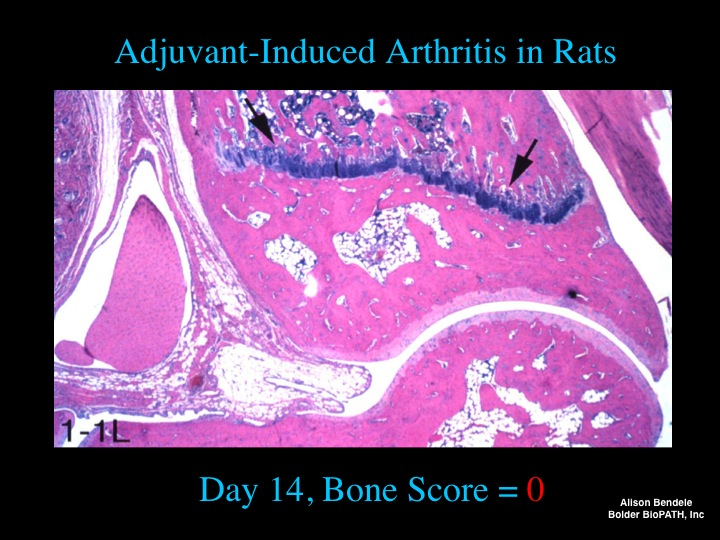
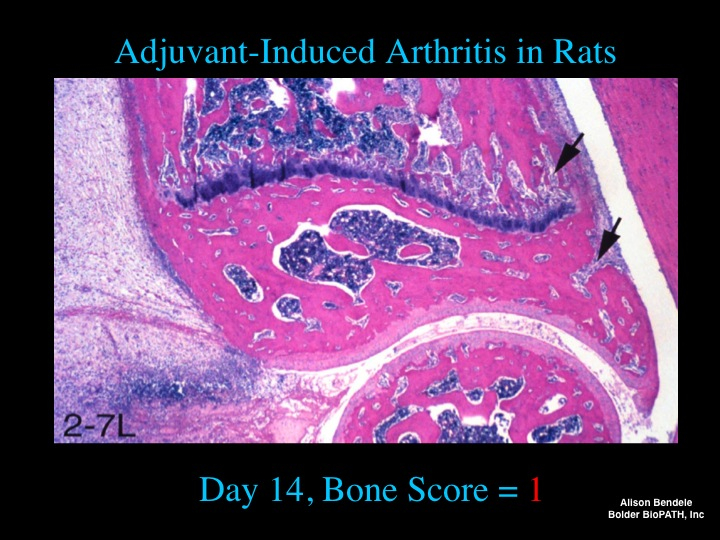
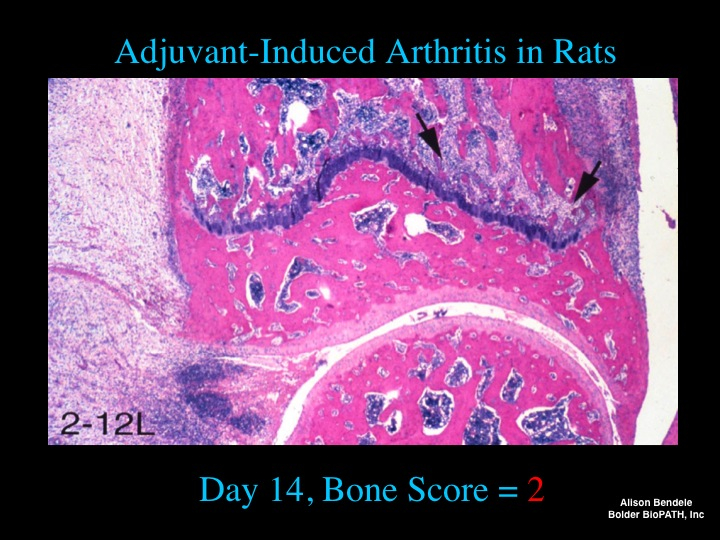
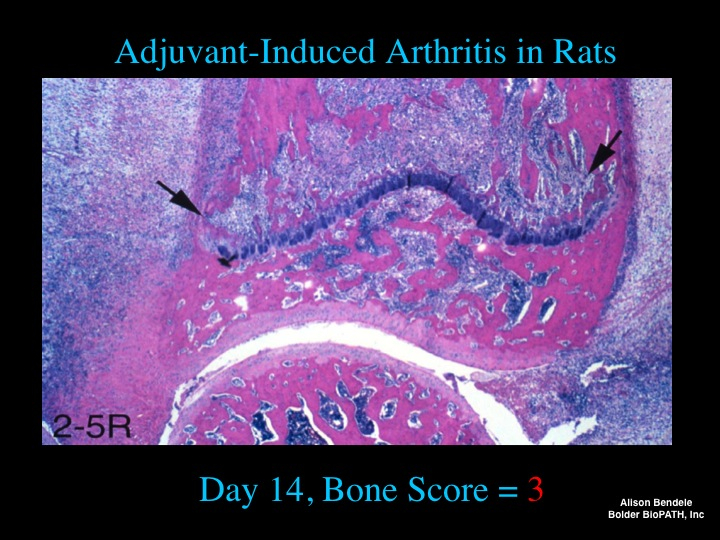
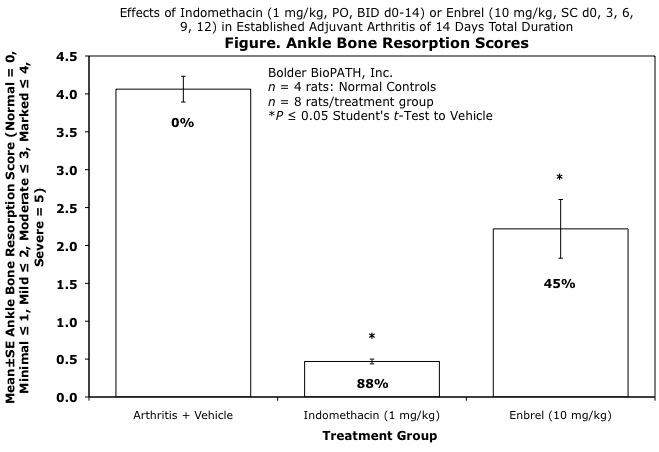
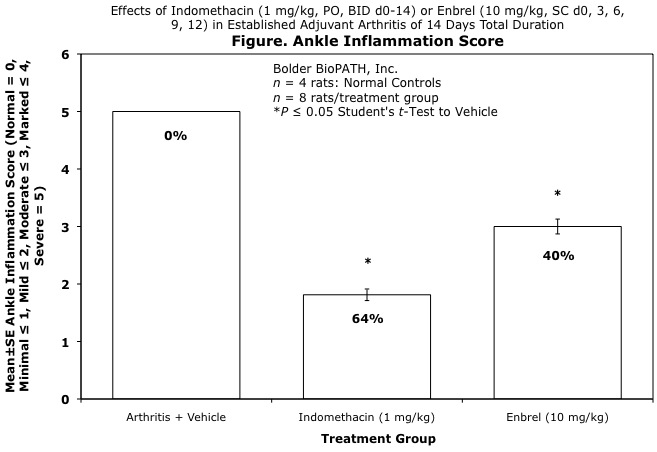
Ankles are given scores of 0 to 7 for inflammation, cartilage damage, pannus formation, and bone resorption according to these methods.
Also, spleens are given scores of 0 to 5 for splenic inflammation, lymphoid atrophy, and extramedullary hematopoiesis according to these methods.
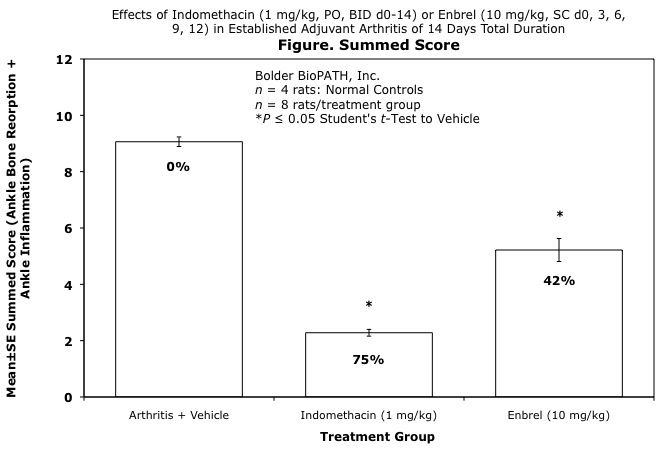
Sample Data (click on image to enlarge):
Photomicrographs: Ankle Bone Resorption